Diagnostic Tests Used for IBD
GI specialists have many resources at their disposal to diagnosis the appropriate IBD sub-type. The modalities that they may use for detecting and monitoring Crohn's Disease include sigmoidoscopy, colonoscopy, double-balloon enteroscopy, small bowel follow through, EGD, flexible sigmoidoscopy, MRE, CTE, capsule endoscopy and the Crohn’s Video Capsule.
The American Journal of Gastroenterology published in 2014 found that small bowel follow-through and CTE scans of the small bowel are valuable, however CTE exposes the patient to radiation and is less accurate for early disease detection in the small bowel.
The Video Capsule - Crohn’s capsule is specifically designed to be used for patients suspected of having Crohn’s Disease. It is intended for visualization of the small bowel and colonic mucosa:
- It may be used in the visualization and monitoring of lesions in the small bowel that may indicate Crohn’s disease not detected by upper and lower endoscopy, and for the visualization of inflammation of the colon in patients with colonoscopy-diagnosed Crohn’s disease
- It may be used in the visualization and monitoring in the small bowel of lesions that may be a source of obscure bleeding (either overt or occult) or that may be potential causes of iron deficiency anemia (IDA) not detected by initial upper and lower endoscopy
- The Crohn’s Video Capsule may be used as a tool in the detection of abnormalities of the small bowel
- It is intended for use in adults
Contraindications:
The Crohn’s Video Capsule is contraindicated for use under the following conditions:
- In patients with known or suspected gastrointestinal obstruction, strictures, or fistulas based on the clinical picture or pre-procedure testing and profile
- In patients with cardiac pacemakers or other implanted electromedical devices
- In patients with dysphagia or other swallowing disorders
- In patients with allergies or known contraindication to the medications and preparation agents used in the procedure as described in the relevant instructions for use
Procedure Risk Information
The risks of the Crohn’s video capsule include capsule retention, aspiration, and skin irritation. The risks associated with colon preparation are allergies or other known contraindications to any preparation agents or medications used for the Crohn’s Video Capsule system regimen, according to laxative medication labeling and per physician discretion. Medical, endoscopic, or surgical intervention may be necessary to address any of these complications, should they occur. After ingesting the Crohn’s video capsule, and until the capsule is excreted, patients should not be near any source of powerful electromagnetic fields, such as one created near an MRI device.
In another study in Clinical Gastrointestinal and Hepatology, capsule endoscopy had a higher sensitivity and specificity as compared to CTE for diagnosing Crohn's Disease. Additionally, this study shows higher yield of diagnostic findings in the proximal small bowel with capsule endoscopy than using either radiologic examinations. The study evaluated 93 patients, comparing the accuracy of capsule endoscopy in patients with newly diagnosed Crohn’s Disease.| Method | Sensitivity | Specificity |
|---|---|---|
| CE | 100% | 91% |
| CTE | 76% | 85% |
| MRE | 81% | 86% |
As physicians strive to get to a diagnosis, many tools, including the Crohn’s Video Capsule, can help doctors help their patients with the medical management of their disease. In Italy, 18 patients with suspected or known Crohn’s Disease, were assessed by CE with the new Crohn’s Video Capsule. In the suspected CD group, approximately one-half of patients had major inflammatory lesions, most of them being in the third tertile (distal portion of the small intestine). In 75% of these patients, the diagnosis was confirmed. In the established CD group, 90% of patients had important lesions in the terminal and neoterminal ileum. No adverse events were reported. Another study made in Israel included 49 patients who were examined by the new capsule in order to assess the system’s capacity to visualize and examine the small bowel and the colon. From 71% of patients who had established CD, 31% of them had proximal inflammatory lesions. All recordings were of good quality, and no retention of the capsule was reported.
Other Modalities
 SBFT: The small-bowel follow-through (SBFT) examination has historically been the standard radiologic approach used to assess patients with active Crohn's Disease (CD), as more than 70% of patients have involvement of the small intestine. However, researchers in some studies have shown that SBFT is not accurate for detection of active CD in the small bowel. It has been suggested that small-bowel enteroclysis is more accurate than SBFT at detecting early mucosal lesions, but both methods provide only limited and indirect information in regard to the state of the bowel wall and extraluminal extension of CD.
SBFT: The small-bowel follow-through (SBFT) examination has historically been the standard radiologic approach used to assess patients with active Crohn's Disease (CD), as more than 70% of patients have involvement of the small intestine. However, researchers in some studies have shown that SBFT is not accurate for detection of active CD in the small bowel. It has been suggested that small-bowel enteroclysis is more accurate than SBFT at detecting early mucosal lesions, but both methods provide only limited and indirect information in regard to the state of the bowel wall and extraluminal extension of CD.
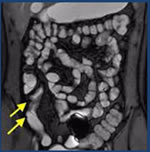
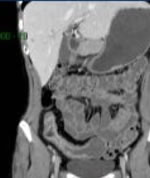 CTE: computed tomographic (CT) enterography has become accepted as a noninvasive imaging technique to evaluate CD. In addition to allowing visualization of extraenteric structures, CT enterography with the use of oral neutral contrast agents and rapid intravenous contrast infusion can be used to reliably identify active inflammation in the small intestine. However, because patients with CD are often young and CD is a chronic and relapsing disease, they may undergo repeated imaging examinations to assess the status of their disease, which exposes them to radiation.
CTE: computed tomographic (CT) enterography has become accepted as a noninvasive imaging technique to evaluate CD. In addition to allowing visualization of extraenteric structures, CT enterography with the use of oral neutral contrast agents and rapid intravenous contrast infusion can be used to reliably identify active inflammation in the small intestine. However, because patients with CD are often young and CD is a chronic and relapsing disease, they may undergo repeated imaging examinations to assess the status of their disease, which exposes them to radiation.
 MRE: magnetic resonance (MR) enterography has been introduced as a radiation-free alternative method to evaluate patients with CD. Investigators in several reports have shown MR enterography to be useful for the identification of active ileitis, assessment of disease activity, and evaluation of extraenteric complications in patients with CD.
MRE: magnetic resonance (MR) enterography has been introduced as a radiation-free alternative method to evaluate patients with CD. Investigators in several reports have shown MR enterography to be useful for the identification of active ileitis, assessment of disease activity, and evaluation of extraenteric complications in patients with CD.
The sensitivity values of CT enterography and MR enterography for the detection of extraenteric complications have shown to be significantly higher than those for SBFT.
GI specialists have many resources at their disposal to diagnosis the appropriate IBD sub-type. CT enterography provides better visualization of the entire small bowel wall and shows extra-enteric complications of small bowel disease. If Crohn's Disease is suspected, capsule endoscopy can provide direct visualization of the small bowel mucosa (where other modalities don’t) and can assist in a more timely diagnosis.
Capsule endoscopy or the Crohn’s Video Capsule would not be used alone for the diagnosis of IBD or Crohn's Disease, but it can provide an initial diagnosis with the use of inflammatory markers, GI or extraintestinal symptoms, and other imaging techniques. This means there is an opportunity to use capsule endoscopy in the treatment and management of Crohn's Disease, to verify therapy is working.
According to the 2015 ASGE guidelines, the authors concluded that capsule endoscopy is useful in the initial diagnosis of Crohn's Disease, for those who have no obstructive symptoms. The authors recommend patency capsule of radiology for those patients with suspicion of an obstruction before a capsule endoscopy procedure. The authors also recommended capsule endoscopy in patients with established Crohn's Disease and unexplained symptoms when abnormalities detected will alter management.
